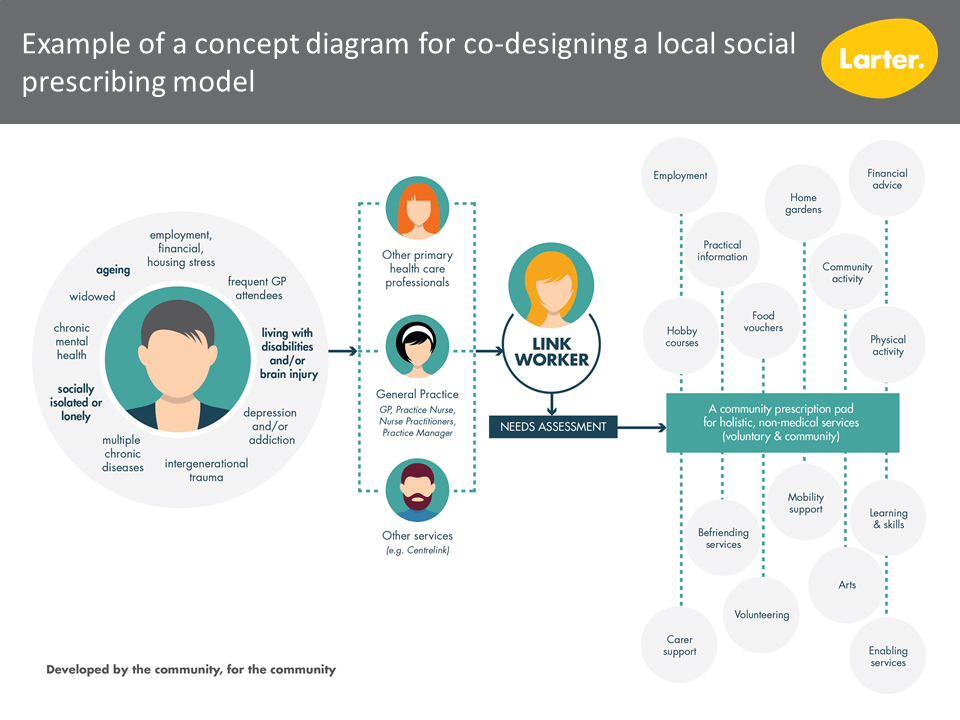
‘Social Prescribing’ is a means to enable health professionals to refer patients to local, non-clinical services and supports. In other words, it is non-medical prescribing that improves health and wellbeing. Examples include community referral to social or physical activities; to a community group; or to learning and skills development activities. A social prescribing program usually involves a clinician connecting the patient/client to a ‘link worker’(also known as ‘community connector’ or ‘navigator’) who works to facilitate the social prescription.
Primary health physicians often talk of not having the time nor resources to be able to fully engage and empower people to address aspects of their lives that are having a significant impact on their mental and physical health.
Social prescribing enables primary health providers to address the wider social determinants of health by referring patients whose health is affected by non-medical factors to community services and supports. These non-medical factors include access to safe and affordable housing; access to learning and skills development; the availability of healthy foods and the capability to prepare healthy meals; financial security/stress; and opportunities to socialise/loneliness. In the Victorian communities we have been working in recently, some of the key priorities for individuals have been: having someone to talk to; working on strengths and goal-setting; and improving self-esteem and confidence.
Social prescribing in the United Kingdom (UK) and New Zealand
Social prescribing has a 25-year history in the UK. It emerged from an initial focus on reducing social isolation in ageing populations, and community renewal programs after industrial decline, in cities such as Liverpool. In response to its increasing applications and building on learnings, the UK government has recently embedded social prescribing into its primary care strategy and has invested in 1,100 social prescribers (one per primary care network).
New Zealand is also known for its innovative approaches such as the Green Prescriptions program to increase the physical activity of largely sedentary people and their families. Through this initiative, General Practitioners provide brief advice then prescribe community walking, exercise and nutrition activities either for individuals or whole families.
Evidence
The evidence base for social prescribing is emerging, and most is from the UK.
At individual level, there is evidence to support
- Improved patient care outcomes, patient satisfaction and quality of life, including
- Improved emotional wellbeing
- Increased confidence and feelings of self-empowerment
- Reduced levels of depression and anxiety
At health system level, there is evidence to support:
- Improved overall efficiency of delivering population level care, including
- Reduced need for GP visits
- Reduced used of prescription medication
- Reduced Emergency Department visits
- Improved provider satisfaction
- Increased integration between health and community support sectors
At community level, there is evidence to support:
- Increased volunteering
- Increased use of community assets
There is further discussion about the evidence base on the King’s Fund website.
Social prescribing in Australia
Similar public health interventions have been trialled in Australia since the 1990s including the Active Script Program in Victoria (physical activity), Lifescripts nationally (smoking, nutrition, alcohol, physical activity) and Indigenous Lifescripts out of James Cook University. Key lessons from these local experiences included:
- The need to have a dedicated worker who could provide motivation, support and ongoing review
- The need for prescribed activities to be free or affordable, and
- That General Practitioners need conversation scripts to support sensitive conversations.
Social prescribing has arrived in Australia in the last two years. There are a number of trial sites testing different approaches in local contexts.
At the moment, the Australian appetite is being driven by individual Primary Health Networks, academia, individual health services and/or community services (e.g. Neighbourhood Houses), and representative stakeholder bodies such as the Royal Australian College of General Practitioners (RACGP) and the Consumers Health Forum of Australia (CHFA).
The interest in Australia is stemming from:
- Policy interest to address the social determinants of health
- The promising outcomes from the UK, especially pertaining to people:
- with one or more chronic conditions
- who need support with their mental health
- who are lonely or isolated
- who have complex social needs that affect their wellbeing.
- The need to address increased demands on GPs and their workload due to increasing presentations for mental illness and co-morbidities.
A national roundtable discussion hosted by the RACGP, CHFA and the Health System Sustainability Partnership Centre in 2019 formulated recommendations to policymakers, funders/commissioners, and service deliverers. The roundtable concluded that based on research in the UK a systematic, nationally scaled and locally implemented approach to social prescribing in Australia could lead to:
- preventing and managing physical and mental illness
- shifting the focus from illness to wellness
- increased consumer enablement and self-management
- decreased demand for health services
- greater value care
- fewer silos between health and community services
- increased joy and decreased helplessness
- decreased isolation and loneliness
- stronger communities.[1]
While social prescribing is relatively new in Australia, Larter has found the sentiment amongst community and health service stakeholders to be very positive and it’s likely that the introduction of a social prescribing program would be welcomed in many communities.
Co-designing local models
In Australian contexts there is not sufficient experience to reach conclusions about how social prescribing might work most effectively. Nor can we currently answer questions about acceptability, community and provider readiness, required partnerships, link worker models and likely broader impact on service systems. What we do know, though, is that models need to be designed to fit particular communities rather than there being a ‘one size fits all’ model across Australia.
Larter has recently worked with a number of communities and clients to co-design local social prescribing models that are fit-for-purpose. This included identifying:
- conditions for effective individual engagement in social prescribing
- support for the engagement of GPs and community service providers
- recommendations about for local service pathways and protocols
- the conditions required to enable increasing uptake
- funding available to models.
We have developed a co-design framework to guide how we work with local general practice sectors, community members, and community services and organisations to identify local enablers, barriers and opportunities.
Click here to go to a list of related case studies.
Some key documents for further reading
Social prescribing: A rapid literature review to inform primary care policy in Australia
‘Iso’ – a spur to think about social prescribing
Are Australia’s GPs ready for social prescribing?
Social and economic impact evidence
- Scoping a feasible and fit-for-purpose model of Social Prescribing for Latrobe Valley
- Macedon Ranges volunteer community support model for mental health and suicide prevention
Links to pilot social prescribing sites in Australia
IPC Health, Deer Park (VIC)
Highett Neighbourhood House – Social prescribing in a Neighbourhood House context (VIC)
Mt Gravatt, Ways to Wellness Social Prescription project (QLD)
Gold Coast ‘Plus Social’ “Not your ordinary prescription” (QLD)
Redland Community Centre – All for One Wellness (A4OW) (QLD)
CheckUP Australia – Lifestyle modification programs – Green Prescriptions (GRx) (QLD)
Plus Social for injured workers – iCare (NSW)
Wentworth Healthcare, Social Connectedness (NSW)
The Waverton Hub, Sydney, Social Prescribing for reducing social isolation and healthy active ageing (NSW)
Contact us to discuss your ideas further or to register your interest in future projects.