Introduction – ‘Making Tracks Together‘
We admire the boldness of Queensland’s ‘Making Tracks Together’ strategy and decided to write a blog – partly as a research exercise to learn more ourselves, and partly to share this initiative with our networks.
A statewide audit of institutional racism
In 2018, an Australia-first investigation into levels of institutional racism in Queensland’s public health system found low levels of Indigenous participation in governance, policy implementation, and service delivery.
The Queensland Human Rights Commission in partnership with Queensland Aboriginal and Islander Health Council (QAIHC) released the influential report Addressing Institutional Barriers to Health Equity for Aboriginal and Torres Strait Islander Peoples in Queensland’s Public Hospital and Services. The report, by Associate Professor Adrian Marrie, found that 10 of the 16 health and hospital services (HHSs) in Queensland that were assessed scored ‘very high’ levels of institutional racism, and the remaining six ‘high’.
The former CEO of Queensland Aboriginal and Islander Health Council (QAIHC), Neil Willmett, said:
A one-off audit and report of this kind is not enough to change the system, but it is a start. Having solid data around levels of institutional racism is particularly helpful in terms of quantifying what Aboriginal and Torres Strait Islander Queenslanders have been anecdotally reporting to us for many years. Obviously, we’d like to see other state health systems take it on board. Queensland is by no means the only state with issues like these1.
This pivotal work would drive the Queensland Government and QAIHC to create Making Tracks Together, the strategic framework to drive health equity and eliminate institutional racism across the public health system in Queensland.
Background
Aboriginal and Torrres Strait Islander peoples are continually striving for improved health outcomes for their communities due to experiencing significant health and social inequities.
As readers will likely know, an Aboriginal Community Controlled Health Organisation (ACCHO) is a primary health care service initiated and operated by the local Aboriginal community to deliver holistic, comprehensive and culturally appropriate health care to the local community through a member-elected Board of Management. QAIHC is the peak organisation representing ACCHOs in Queensland at both a state and national level. ACCHOs are independent of Queensland Health.
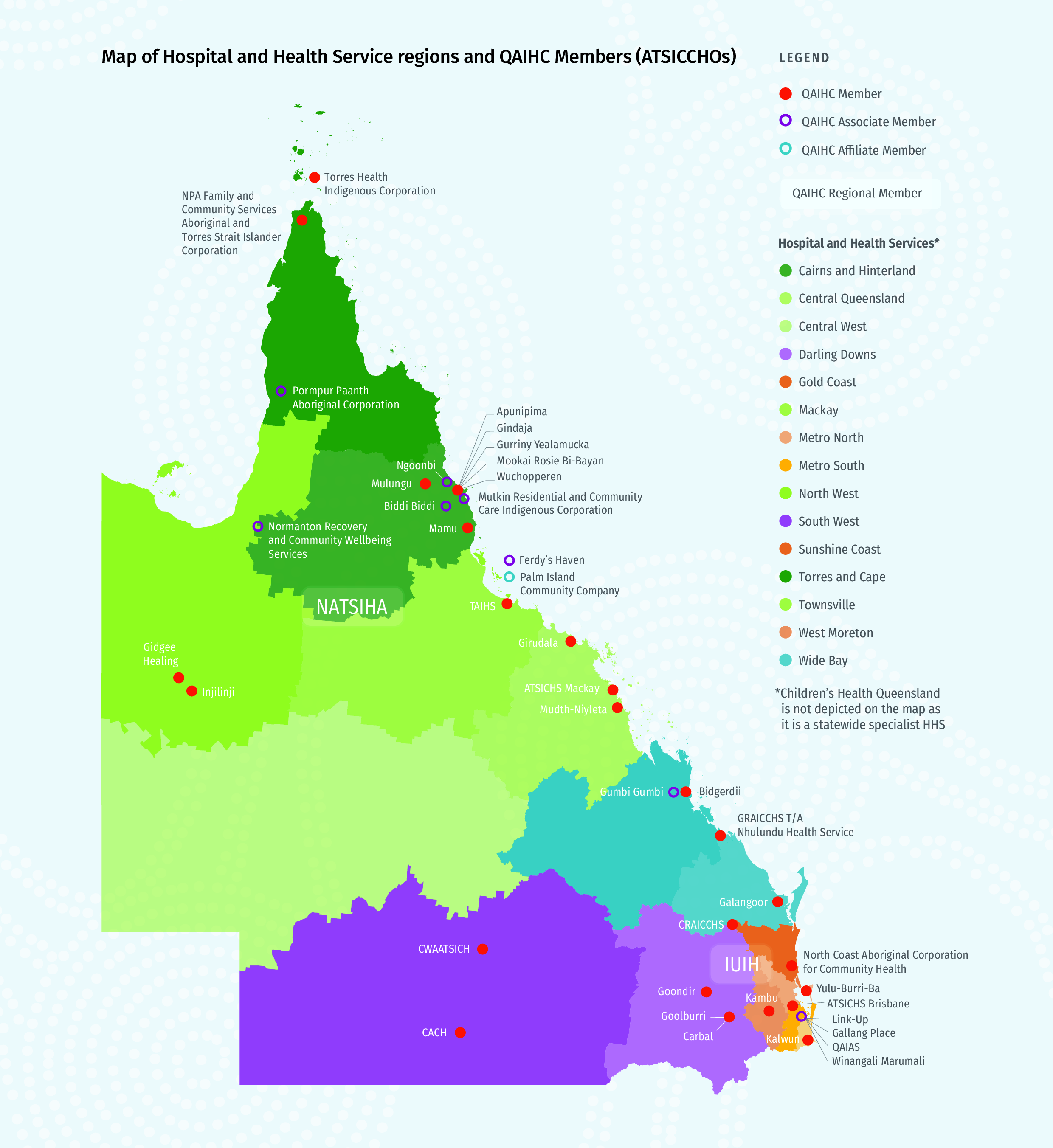
In Queensland, public health (including hospitals) is governed through 16 regional hospital and health service (HHS) boards. Each HHS has a service agreement with Queensland Health, who provides funding and defines how performance needs to be monitored.
Below is a map of HHS regions, and ACCHOs.
Policy Origins
In 2010, QAIHC partnered with the Queensland Government to launch the state’s first health equity strategy, Making Tracks toward closing the gap in health outcomes for Indigenous Queenslanders by 2033: Policy and Accountability Framework.
This comprehensive, evidence-based policy framework aimed to provide the policy directions to guide the Queensland Government’s effort to achieving health parity between Aboriginal and Torres Strait Islander peoples and non-Indigenous Queenslanders.
In 2017, Anti-Discrimination Commission Queensland (now the Queensland Human Rights Commission) and QAIHC commissioned the report, Addressing Institutional Barriers to Health Equity for Aboriginal and Torres Strait Islander Peoples in Queensland’s Public Hospital and Services. This Australia-first assessment on levels of institutional racism in Queensland’s public health system found low levels of Indigenous participation in governance, policy implementation, and service delivery. This pivotal work sparked legal and regulatory changes, focusing on how to overcome institutional racism.
The report used a tool, known as the ‘Marrie Institutional Racism Matrix’ (the Matrix) to provide a set of baseline data from which to measure progress towards elimination of institutional racism in health services over time.
Institutional racism has been defined by the Australian Hospitals and Healthcare Association (AHHA) as hidden racism that enables organisations to deliver unequal outcomes for some groups in society. It comes about due to the way organisations are governed, staffed, resourced, operated, and held accountable. Excluding certain groups from these aspects can lead to poorer outcomes for that group. Independence from staff prejudices or actions is important because training and development will not improve matters.3.
The report found that 10 of the 16 health and hospital services (HHSs) in Queensland that were assessed scored ‘very high’ levels of institutional racism, and the remaining six ‘high’.
The audit provided solid data for Queensland Health to implement a number of strategies to address institutional racism in the health system, including the Statement of Action toward Closing the Gap in health outcomes and Closing the Gap Health Plans.
On 26 October 2021, Making Tracks Together (with the addition of the word ‘Together’) was co-launched by the former Minister for Health and Ambulance Services, the Hon Yvette D’Ath, and QAIHC’s Chairman Mr Matthew Cooke. This is now Queensland’s Aboriginal and Torres Strait Islander Health Equity Framework.
Making Tracks Together was released to support hospital and health services to develop and implement health equity strategies. The strategies outline the actions each hospital and health service will deliver to achieve health equity, actively eliminate racial discrimination and institutional racism, and influence the social, cultural and economic determinants of health by working with Aboriginal and Torres Strait Islander organisations, health services, communities, consumers and Traditional Owners.
A brief overview of Making Tracks Together
Priorities
- Priority 1 – A healthy start to life: Ensuring Aboriginal and Torres Strait Islander children 0-8 years are best placed for a healthy and safe start to life.
- Priority 2 – Addressing risk factors: Addressing the modifiable risk factors that contribute to preventable and chronic conditions.
- Priority 3 – Managing illness better: Establishing seamless pathways facilitating enhanced access to screening, early diagnosis, procedures and appropriate treatment of chronic conditions.
- Priority 4 – Effective health services: Improving Aboriginal and Torres Strait Islander peoples’ access to, and experience in, the health system, ensuring cultural capability throughout the patient journey and across the healthcare continuum.
- Priority 5 – Improving data and evidence: Improve the quality and availability of research, data, accountability mechanisms and evaluation.
See – First Nations Health Equity | Queensland Health
Objectives and principles. The primary objective of Making Tracks Together is to minimise health inequities by addressing the social determinants of health including education, employment, and living conditions. Emphasis is placed on prevention, improved management of chronic conditions, increased accessibility to effective health services, and use of research and data. The strategy also aims to amplify cultural competency and reduce racism.
A critical principle is partnership between communities, public health services and ACCHOs. Cultural respect is highlighted as an important pillar of competent health services. A holistic definition of health is recognised – encompassing the physical, spiritual, cultural, emotional, and social well-being of individuals and their communities. The principle of community control of primary health care services is also recognised.
The Evolution of ‘Making Tracks Together’
Over the years, the policy has incorporated lessons from regional experiences and has adapted:
- In 2011, each HHS was mandated to ensure Aboriginal and Torres Strait Islander peoples representation on its Board
- In 2021, each HHS was mandated to develop and publish a health equity strategy for Aboriginal and Torres Strait Islander peoples
- In 2021, Queensland introduced minimum requirements for Health Equity Strategies – including co-design, consultation on draft strategies, decision making, conflict resolution, and guidance on key performance indicators.
There is a strong focus on HHSs working to eliminate racial discrimination and institutional racism such as by reviewing policies, employing more First Nations people, and measuring change.
Is there anything missing?
Aboriginal and Torres Strait Islander people continue to suggest changes at both regional and state levels.
Toombs, Curtis and Brolan4 stated digital accessibility (and the digital determinants of health) may need stronger consideration. They also remind us that access to public health services should not be a KPI but is in fact a fundamental human right enshrined within the Human Rights Act 2019 (Qld).
Intergovernmental relationships (i.e., between state, local and federal) may also need a stronger focus. For example, the federal government is deeply involved in health, housing, and communications, to name just three areas. Local governments, including shires controlled by Aboriginal and Torres Strait Islander people, are actively involved in housing, early childhood services, and local infrastructure planning.
Examples of HHS Health Equity Plans
Within the scope of the Making Tracks Together health equity strategy, all HHSs have now published their strategies. Below are some examples:
A. Metro South Region, Brisbane
- The traditional custodians of the land and water of the region are the Yugambeh, Quandamooka, Jaggera, Ugarapul and Turrbal peoples
- The Consultation report identified the following key needs:
- Provision of culturally safe health care
- Provision of health services that are completely free from racism and discrimination
- Engagement with First Nations people before designing healthcare systems
- Reform public services to fully meet population need – e.g. there is a lack of access to Indigenous Health Liaison Officers, including after-hours services in some cases
- Access to public specialist primary health services in Logan and Beaudesert.
- Two-page Strategy and Implementation Plan – First Nations Health Equity Strategy 2022-2025 | Metro South Health
- The implementation plan has six priority areas:
- Actively eliminate racial discrimination and institutional racism within the service
- Increase access to healthcare services
- Influence the social, cultural, and economic determinants of health
- Deliver sustainable, culturally safe, and responsive healthcare services
- Work with First Nations peoples, community and organisations to design, deliver, monitor and review health services
- Strengthen the First Nations health workforce.
B. Cairns and Hinterland Region
- The traditional custodians of the land and water of the Cairns and Hinterland region are the Gimuy Walubara Yidinji people, along with other various tribes within the Bama Rainforest Peoples.
- More than 30 consultations were conducted with over 170 stakeholders.
“Our Indigenous peoples have been ‘doctors’ since time, our Indigenous peoples should be at the forefront of this Health Strategy.”
Comment from a community member
- Discussion points during consultations included:
- the need for more transport, housing, support services
- access to fresh fruit and vegetables
- greater respect
- increasing cultural capability including by employing more First Nations staff
- more collaboration to improve and evaluate services including between primary and acute care.
- The key priority outcome areas are:
- Improving health and wellbeing outcomes
- Actively eliminating racial discrimination and institutional racism within the service
- Increasing access to healthcare services
- Influencing the social, cultural and economic determinants of health
- Delivering sustainable, culturally safe and responsive healthcare services
- Working with First Nations peoples, communities and organisations to design, deliver, monitor and review health services.
- First Peoples Health Equity Strategy | Cairns and Hinterland Hospital and Health Service – this inaugural Strategy has been dedicated to the health equity research work of Henrietta and Adrian Marrie, and to all First Peoples who have encountered and fought to end racial discrimination in health care.
C. Other strategies
Other HSS strategies can be accessed here.
Conclusion
Queensland’s First Nations Health Equity Strategy is a groundbreaking initiative that has legislative force. Of course, legislation and regulation can only go so far – it will be the extent of commitment and skill of local and regional leaders to turn plan to reality.
If successful – and we genuinely hope it is – this comprehensive approach to health equity (from fostering a diverse workforce, implementing measures to eliminate institutional racism, to co-designing health services with community involvement) has potential to transform the health landscape through genuine co-design, action and monitoring.
Monitoring and evaluation of regional strategies will be critical for both accountability and to offer new opportunities to keep improving, not only in specific regions but in other regions through the sharing of what’s worked well and what hasn’t. A key positive is the willingness to keep evolving the Making Tracks strategy over time.
References
- Queensland Aboriginal and Islander Health Council. (n.d.). Audit finds high levels of institutional racism in Queensland’s health system, but experts hopeful of brighter future. Retrieved from https://www.qaihc.com.au/
- State of Queensland (Queensland Health), Queensland Aboriginal and Islander Health Council. (2021). Making Tracks Together Queensland’s Aboriginal and Torres Strait Islander Health Equity Framework [PDF]. Retrieved from https://www.health.qld.gov.au/__data/assets/pdf_file/0004/150687/health-equity-framework.pdf
- Bourke, C. (n.d.). Institutional Racism in Australian Healthcare Settings. Retrieved from https://aci.health.nsw.gov.au/__data/assets/pdf_file/0003/555807/Institutional-racism-in-Australian-hospitals-and-healthcare-settings.pdf
- Toombs, M., Curtis, C., & Brolan, C. (2023). Supporting Indigenous health equity strategic planning: a Queensland perspective. Medical Journal of Australia, 218(1), 5-8.